Posts Tagged ‘pandemic’
The COVID-19 pandemic is pushing teachers and public education to the brink of collapse
By Katie Hudson, PhD

There is no question that the COVID-19 pandemic has taken a devastating toll on K-12 students in the U.S. and in a deeply politically polarized country, there is broad consensus that children have fallen behind, their well-being is suffering, and something needs to be done.
- Standardized test results from the 2020-21 school year show that student achievement was lower in all measured subjects and demographics, especially in math and for young, low-income, or minority children.
- The number of chronically absent students has nearly doubled.
- Crying and disruptive behaviors at school have increased in younger children, while bullying and violence have increased among teenagers.
- Despite most students learning remotely at the beginning of the year, there were at least 42 school shootings reported in 2021, shattering the previous record of 30 school shootings in 1999.
- Suicide attempts among teenagers in 2020 increased 31% from the previous year and were 51% higher for teenaged girls in early 2021 compared to the same time period in 2019.
- School psychologists are facing a “river of referrals” and because they are already understaffed, they do not have time for long-term planning to promote better mental health within their schools.
- The American Academy of Pediatrics declared a National Emergency in Child and Adolescent Mental Health in October 2021 and noted that over 140,000 children had lost a primary and/or secondary caregiver due to COVID-19.
Evidence emerged that children were less susceptible to COVID-19 and school districts began to resume in-person instruction: only 40% offered in-person options at the beginning of the 2020-21 school year and over 98% provided in-person options at the end. The U.S. media has increasingly delivered the message that the pandemic has created a crisis for American children, children are less susceptible to COVID-19, and therefore K-12 schools need to resume in-person teaching. However, the calls to action often fail to consider the most fundamental requirement to resume in-person schooling: teachers.
Prior to the pandemic, the U.S. already faced a national teacher shortage and protests from teachers for better pay and support. The profession is notorious for being low-income, long hours, and undervalued in U.S. society. All states require teachers to hold a bachelor’s degree and undergo additional state-specific certifications and licensing prior to teaching in public schools, and more states are now adding master’s degree requirements. Nearly half of all teachers borrow an average of $56k in loans to pay for their degree and still owe roughly $60k due to high interest rates and low salaries. Many were enticed by the federal Public Service Loan Forgiveness program that promises loan balance forgiveness after making around 10 years of qualifying payments; however, 98% of applicants for this program are rejected for minor and often nonsensical technicalities. Despite providing such an essential service for future generations, many teachers struggle to financially support themselves and are forced to work additional jobs. U.S. teachers also have more students and spend significantly more time teaching compared to teachers in other countries, leading to less time for other tasks like staff meetings, planning, grading, parent conferences, and career development activities. Studies show that higher teacher pay and societal status are strongly correlated with student outcomes and that “the perceived value of the teaching profession by society is important in attracting, recruiting and retaining high-quality teachers”.
When U.S. school districts began requiring teachers to return to their physical classrooms for the beginning of the 2020-21 school year, many teachers opted for early retirement or resignation and teachers with more years of experience left at higher rates than less experienced teachers. Over 30% of teachers have retired since the onset of the pandemic. In a survey of government employees conducted in May 2021 (i.e., before the Delta and Omicron variants emerged in the U.S.), nearly half of teachers indicated that in-person work posed a risk to their health. When compared to all other government employees, teachers were significantly more likely to (1) report that the risks they were taking during the pandemic were not proportionate with their compensation; (2) experience stress, burnout, and/or fear due to COVID-19; and (3) be negatively financially impacted by the pandemic.
The U.S. is the only country in the world that does not include guaranteed worker pay in their national leave policy. Out of the 193 UN members, the U.S. is one of only ten members that do not offer some form of paid sick leave to reduce infectious disease spread. The U.S. passed the Families First Coronavirus Response Act at the onset of the pandemic and required employers to provide paid sick leave for COVID-19-related reasons, but it expired on December 31, 2020, and the only provision that congress temporarily extended was a tax incentive for employers who voluntarily provided paid leave. It is currently up to states and local jurisdictions to establish any pandemic-related paid leave policies and these widely vary between states. Many teachers already receive a low number of annual sick days and some districts are not giving teachers additional paid leave if they catch COVID-19, forcing teachers with limited remaining personal sick days to choose between going without pay or teaching while infected; since most are already financially struggling, they are often forced to choose the latter. A Missouri superintendent stated “The more COVID leave you offer, the more likely it is people will use that leave, which then increases your substitute costs.” This type of disregard for teacher health and safety from school leaders has been felt by a variety of school workers and is further contributing to staff shortages.
In addition to feeling like their health and safety are disregarded by their administrators, teachers are also forced to face parents that protest or refuse to comply with their school’s safety mandates. Open house events and the first week of the 2021-22 school year were especially difficult:
- An Illinois principal asked a mother to adjust her mask to cover her nose. The mother refused, was asked to leave the school property, continued to refuse, and was eventually arrested. The mother then bragged on social media about her actions and subsequent banning from school property.
- A Texas school district had one teacher yelled at for wearing a mask and another teacher had her mask ripped off by a parent.
- A California teacher was hospitalized on the first day of school after being physically attacked by a parent who referred to masks as a “conspiracy”.
- A Florida father, whose daughter was turned away on a daily basis for not wearing her mask, assaulted another student at his daughter’s school.
As if fights with parents were not enough, the politicization of the pandemic has led to some elected officials crippling a school’s ability to enforce any safety mandates. In 2021, Republican governors in 8 states issued executive orders to banschool mask mandates. When some schools refused to comply, several governors enacted additional legislation that financially punished the districts that continued to enforce mask mandates. Arizona’s governor Doug Ducey announced a $163 million program to increase funding to schools that followed the law (i.e., schools that required masks would not receive the extra funding) and a separate program to financially assist families in leaving districts with mask mandates and other COVID safety measures. Florida’s governor Ron DeSantis went even further by withholding already-allocated state funding for districts with mask mandates. The Department of Education sent letters to these 8 governors to admonish them for blocking their schools “from voluntarily adopting science-based strategies for preventing the spread of COVID-19 that are aligned with the guidance from the CDC” and for instituting policies that did not align with the $122 billion funds distributed to states as part of the 2021 American Rescue Plan to assist schools in safely reopening. Virginia’s recently elected Republican governor Glenn Youngkin issued an executive order in January 2022, making Virginia the 9th state to hinder school mask mandate enforcement. Youngkin has also established a ‘tip line’ for Virginians to inform his administration of teachers who violate any of his orders, which has understandably led to teachers feeling intimidated and unnecessarily targeted. Policies that go against science to address perceived cultural grievances that are not actually happening are increasingly being proposed across the country and are making it more difficult for teachers to perform their work. “It’s just created an environment that people don’t want to be part of anymore,” said the Executive Director of the American Association of School Administrators. “People want to take care of kids, not to be accused and punished and criticized.”
How can we attract and retain more qualified K-12 teachers? When asked how their employer could make their workplace a better place to work, public school teachers most frequently recommended promoting safety, following CDC guidelines, and providing and/or enforcing PPE use in their school; the next most frequent responses were issuing raises/bonuses and allowing flexibility with hours and remote work. Teachers’ unions have helped educators gain rights such as fair working conditions, adequate compensation, pay equality, tenure mechanisms, and benefits; however, many states have laws that make it difficult or illegal for teachers to form unions or any form of collective bargaining. The pandemic has exacerbated underlying problems in public education and has exposed its weaknesses; unless major reform is enacted – and society pushes for it – we are facing a collapse of the U.S. public education system. A recent Forbes article aptly titled ‘Why Education Is About To Reach a Crisis of Epic Proportions’ stated that “we’re at a major tipping point in education. […] it’s not sustainable. And as a nation, we’re about to feel it.” McKinsey & Company stated last year that “the deep-rooted challenges in our school systems predate the pandemic and have resisted many reform efforts […] The immediate imperative is to not only reopen schools and recover unfinished learning but also reimagine education systems for the long term.” A 2021 brief from the Center for School and Student Progress stated that “next year cannot be a “normal” year. We cannot return to the classroom and do things the same as they have always been done and expect to see a different outcome. Instead, we must use this critical moment in education to radically rethink how programs, policies, and opportunities are designed and fiercely commit to prioritizing the communities most impacted by the pandemic and distributing resources accordingly.”
~
In preparation for writing this article, I spoke with a few local K-12 teachers and posted on several social media platforms with the hope to reach additional teachers in other states. To say that their responses were heartbreaking is a gross understatement. It was readily apparent that each had an immense passion for teaching, but they are at their breaking points (or are already past that). Because the uniting response from these teachers was feeling like they had no voice and that the general public is unaware of what they are going through, it would be a disservice to not include some of their perspectives and experiences. Below are some common responses, as well as a few specific examples that stuck out:
- The media is not accurately depicting what appears to be an inevitable collapse in public education unless major reform is enacted.
- Teachers are being forced to risk their personal health and in return, are met with disrespect, vulgarity, and sometimes violence.
- Teachers are not able to speak up for themselves or do what is right for their families without facing retaliation. Administrators are doing what is best for administrators, not what is best for the teachers and often not even what is best for the students.
- Low-income children are suffering.
- Nothing will change until better politicians are elected, or when the rich politicians’ children are affected like the low-income children.
- The stress they are being forced to endure is hindering their ability to function in their professional and personal lives.
- COVID-19 protocols are not taken seriously at their school or are unclear to staff. Students with close contact or positive test results are not quarantining.
- Teachers who test positive are pressured to keep silent or not undergo testing in the first place when feeling sick because of extreme staff shortages.
- Before the winter 2021 break, in-school testing services refused to test teachers unless they had made an appointment 3 days in advance – which was near impossible due to sporadic and inconsistent scheduling that was not communicated to teachers. Teachers assumed that this was a way to keep in-school case numbers down.
- Teachers were promised masks, but were later told by their principal that there were not enough. Local media continued to report that all teachers were receiving masks.
- Title I school in a rural, low-income area: most kids have behavioral problems, won’t wear their masks, refuse to follow the school’s COVID policies, and will lick and cough on her things because like their parents, they think the pandemic is a joke.
- Parents are not consistently being notified when someone in their child’s class tests positive and therefore that their child was exposed.
- A significant portion of their class just does not come to school anymore.
- There are not enough substitute teachers and educational requirements are being lowered to increase applicants. Teachers do not want to create extra workload for their coworkers since they are all already drowning, so they are not taking any time off.
- Special education students have not received their specialized instruction for the past year because there is no teacher, which is egregious and illegal.
One teacher wanted to share her poem to let other teachers know that they are not alone in their feelings. To quote her ending:
“The job is twisting what teaching should be. The job is twisting me. I am not this job, I am a teacher. I am tired.”
Science Policy Around the Web, January 20, 2022
By Jenna Alkhatib

Omicron forces us to rethink COVID-19 testing and treatments
As the globe makes its way past the second year of the COVID-19 pandemic, there seems to be no shortage of public health challenges presented. Expectedly, the situation is evolving – or mutating, in the case of the Omicron variant. With 60 mutations compared to the original virus, including 32 mutations in the spike protein gene, the Omicron variant has gained some capacity to evade the immunity provided by prior SARS-CoV-2 exposure (although vaccines based on the originally-identified SARS-CoV-2 strain still provide high-level protection). While the Omicron variant is shown to be less severe in terms of causing serious health consequences, the current surge in cases demonstrates it is more transmissible. This has resulted in high-rates of hospital admissions, especially of vulnerable patients, i.e., those who are unvaccinated, immunocompromised, elderly, or with underlying health conditions.
Testing, and isolating when needed, are two key methods for preventing SARS-CoV-2 transmission and reducing rates of hospitalization. Molecular PCR testing and rapid antigen testing have become common household names within the past months due to their abundant utility. Rapid antigen tests are known for their ability to detect whether an individual is infectious to others around them, whereas PCR tests can detect infections before an individual is in their infectious period. However, a recent non-peer reviewed study, published by medRXiv.org, reports rapid antigen tests producing false negative results during the first two days of infection, despite 28 of the 30 tests being classified in the infectious viral load range of Omicron transmission. The findings of this preliminary study imply that Omicron cases may be infectious days before being detectable by rapid antigen tests. Moreover, location and technique of the swabbing for the test may have an effect on the result, as Omicron may be more abundant in the upper respiratory areas, such as the throat, rather than in the nose in the earlier days of infection.
Regardless of the nuances of testing, however, rapid antigen tests still serve their purpose for speed and convenience. As false positives are rare, rapid tests can quickly identify infectious cases of COVID-19, allowing individuals to take immediate precautions to prevent further transmission. All things considered, testing remains an essential tool for limiting SARS-CoV-2 spread and preventing disease.
(Tina Hesman Saey and Laura Sanders, Science News)
Science Policy Around the Web, November 11, 2021
By Tam Vo, PhD

The United States has stopped funding virus research it defines as risky
The NIH recently removed from its website most mention of the words “gain of function” (GOF), a term referring to experiments where scientists modify pathogens to become more infectious or transmissible. NIH stated that the reason for the changes was the terms misuse, as well as confusion around federal rules adopted in 2017 that require a subset of GOF studies to go through a detailed review. This includes studies of “enhanced potential pandemic pathogens” (ePPPs) that, as defined by federal officials, might enhance a pathogen so that it could cause a pandemic. This change came about as a result of a lengthy debate within the Department of Health and Human Services (HHS), NIH’s parent agency.
In 2011, two studies aiming to modify the H5N1 influenza virus variant to be more transmissible to ferrets, were deemed to involve a PPP. The first study was led by Yoshihito Kawaoka at University at Wisconsin, Madison, and the other by Ron Fouchier at Erasmus Medica Center in the Netherlands. The uproar from scientists concerned about a potential virus leak from the lab led to a temporary pause in NIH funding and revisiting the policy for research involving risky viruses. The two studies were briefly resumed in 2019 and then met their end in 2020.
Critics say that the definition of ePPP should be broadened to apply to U.S.-funded coronavirus research at the Wuhan Institute of Virology in China. Although ending NIH-funded ePPP research won’t stop the debate over risky virus research, NIH officials said they are open to re-visiting the 2017 policy, which might change the ePPP definition in the future.
(Jocelyn Kaiser, Science)
Science Policy Around the Web September 16, 2021
By Silvia Preite, PhD

The COVID-19 pandemic has delayed cancer diagnoses and might worsen prognoses
The initial wave of the COVID-19 pandemic led to significant delays in cancer diagnosis and treatment for many patients. This setback was due to a combination of overloaded health care systems and peoples’ hesitancy to visit hospitals. Although diagnostic rates have rebound, the impact of this delay on cancer screening remains unclear.
A new study published in JAMA Oncology has revealed an association between the first 55-day mandatory COVID-19 lockdown in France in 2020, and tumor burden in metastatic colorectal cancer patients. The study examined 80 patients – 40 who underwent screening before the pandemic, and 40 who underwent screening afterwards – and found those diagnosed after the lockdown had a seven times higher tumor burden than those diagnosed before. Median survival of those diagnosed after the lockdown was also decreased by half. Interestingly, the initial aim of this study was to analyze tumor DNA circulating in the blood for genetic mutations critical to respond to targeted therapies. Surprisingly, the authors found higher levels of circulating tumor DNA in most patients diagnosed after resuming the screening activities.
Other diagnostic centers and hospitals worldwide have also reported drastic drops of cancer screening for breast, colorectal, lung, pancreatic, cervical, gastric, esophageal, and prostate cancer during the pandemic. Overall, it will take years to fully appreciate the impact of the COVID-19 pandemic on different types of cancer screening and care with downstream effects on disease outcome and mortality. This work highlighted the importance of early detection, the need to maintain diagnostic programs during a pandemic, and the need to reduce patients’ fears to visit healthcare facilities through a suitable communication campaign.
(Elizabeth Cooney, STAT News)
Science Policy Around the Web July 27, 2021
By Somayeh Hooshmand, PhD

CDC reverses indoor mask policy, saying fully vaccinated people and kids should wear them indoors
The Centers for Disease Control and Prevention suggested that fully vaccinated people who live in high-transmission communities should wear masks indoors again. The CDC is also recommending that all school children wear masks in schools this fall.
The agency has updated its COVID-19 guidance for the Fall. While the super-contagious delta Covid variant is circulating in the United States, many are expecting to see another big, national surge as social activity increases and many offices plan to bring workers back.
CDC Director Dr. Rochelle Walensky said, “This pandemic continues to pose a serious threat to the health of all Americans. Today, we have new science related to the delta variant that requires us to update the guidance regarding what you can do when you are fully vaccinated.”
In mid-May, the CDC said fully vaccinated people can resume activities in most settings without wearing a mask. But with the delta variant, everyone, including the fully vaccinated particularly if they are immunocompromised or at an increased risk for severe disease from COVID-19, should continue wearing masks indoors in certain areas.
Experts still believe fully vaccinated individuals are less likely than unvaccinated persons to get COVID-19 or to spread it to others. However, new data has shown that the delta variant of COVID-19 can be contracted by vaccinated people, who can then transmit the virus to others.
Dr. Walensky said, “The Delta variant behaves uniquely differently from past strains of the virus that cause COVID-19, indicating that some vaccinated people infected with the Delta variant may be contagious and spread the virus to others.”
We have been living with coronavirus exhaustion for months, and covid cases are rising again in the U.S as the delta variant rapidly spreads. It will take all of us, both vaccinated and unvaccinated, to help stop the spread of new variants, even if that means wearing a mask in public.
(Berkeley Lovelace Jr. CNBC)
Pandemic preppers: an overview of the scientific efforts to prepare for the next pandemic
By R. Elliot Murphy, PhD

In the latter months of 2002, SARS-CoV spread throughout east Asia and quickly made its way across the borders of multiple countries around the world in the span of a few months. Severe acute respiratory syndrome (SARS), the disease caused by this new virus was defined by severe flu-like symptoms, an incubation period of 4 to 6 days, and a mortality rate of roughly 10%. The spread of the virus lasted around one year and would claim the lives of nearly 800 people before it was contained.
In the year leading up to the 2016 Olympic games, Brazil was dealing with an outbreak of Zika virus that was spreading across the Americas at a rapid pace. Even though concerns that Zika would spread around the world through Olympic related tourism were largely not borne out, the virus, which causes devastating neurological disorders in newborn infants from infected mothers, wreaked havoc amongst the poorest and most vulnerable populations living in crowded urban districts of south and central American countries.
In 2019, a strain of coronavirus soon to be known as SARS-CoV-2, originated in Wuhan, China, and swiftly spread across the globe, sparing not a single country and upending daily life for almost every person on earth. Covid19, the disease caused by this virus, has killed 2.8 million people at the time of writing.
Though some have been more severe than others, these are just three examples of more than a dozen zoonotic viral epidemics in only the last two decades. Data clearly suggests that zoonotic disease outbreaks have been steadily increasing at an alarming rate over the past half-century. Much like global climate change, these trends can likely be attributed to anthropogenic land-use changes such as urbanization, increased agricultural activities, and the inevitable deforestation that accompanies them. The risk of animal to human transmission of RNA viruses is particularly high due to their ability to adapt to environmental pressures through rapid genetic mutation. Combined with the increased affordability and speed of air travel, the fact that humans show no signs of slowing the current pace of land use changes indicates that, like climate change, the threat of epidemics from zoonotic pathogens will continue to increase over time. Though it may be hard to imagine, it seems likely that the events of the past year will recur in some form. Much like climate change, there may be no going back in terms of undoing the underlying causes of this problem. In order to mitigate the human suffering and economic toll caused by future pandemics, it is imperative that we begin crafting policy and reallocating funds in preparation.
Ostensibly, the prospect of preparing for a pandemic which could originate from any number of pathogenic sources sounds like an impossible task. However, many scientists who study these diseases believe that there is plenty that can be done with technology currently available. Techniques like consensus polymerase chain reaction (cPCR) and next-generation sequencing (NGS) combined with diligent monitoring of high threat-level pathogens may allow for the procurement of consensus genetic sequences. These, in turn, can be utilized as targets in developing vaccines or drugs which are broadly active against the virus family as a whole. However, due to the low market potential associated with drugs and vaccines for newly emerging pathogens, these projects are often poorly funded and stall in early development, and pharmaceutical companies are likewise unmotivated to take up projects in preparation for future pandemics. Nevertheless, various organizations, operating with funds from both public and philanthropic sources, have materialized in recent years to provide ignition capital for these types of projects where funding is lacking.
Perhaps the most well-known and well-funded group working toward this goal is the Coalition for Epidemic Preparedness Innovations (CEPI). This foundation, which was founded in 2017 at the World Economic Forum in Davos, is funded by both public and private sources including the Bill and Melinda Gates foundation and a small consortium of nations comprised of Norway, Japan, Germany, the European union, Britain, Belgium, Canada and Australia. The Stated mission of CEPI is “to is to accelerate the development of vaccines against emerging infectious diseases and enable equitable access to these vaccines for people during outbreaks.” CEPI has chosen to focus its efforts on the World Health Organization’s (WHO) blueprint priority pathogens, a list of diseases compiled and updated annually by a panel of experts that represent the greatest threat in terms of their epidemic potential. CEPI often uses their funds to advance projects that would reduce the time needed to develop a therapeutic response should any of these viruses lead to an epidemic. For example, they donated $25 million in 2018 to kickstart a Nipha virus vaccine trial. The Nipha virus currently has no available vaccine or drug treatments, but phase 1 of the current vaccine candidate is expected to be completed in 2021. Research and design (R&D) are the largest temporal and monetary barriers in terms of creating vaccines and drugs for emerging epidemics. In order alleviate the burden imposed by the R&D process, CEPI has recently launched a $3.5 billion plan which they hope will allow vaccines for future epidemics to be developed in just 100 days.
There are also multiple examples of government funded programs in the United States with goals related to epidemic preparedness. The National Institute of Allergy and Infection Diseases (NIAID) has awarded 11 grants to establish the Centers for Research in Emerging Infectious Diseases Network (CREID Network) which is currently composed of 11 centers in various locations around the globe, including areas where emerging infectious diseases are likely to originate. The primary focus of CREID is to determine which animal populations harbor pathogens likely to spill over into humans and to better understand the genetic traits that make zoonotic transmission possible so that we can respond expeditiously to outbreaks when they occur. The Antiviral Drug Discovery and Development Center (AD3C) is one of the Centers of Excellence for Translational Research (CETR), also funded by NIAID, which focuses on discovery and refinement of small molecule inhibitors, mostly for viral polymerases from emerging pathogens as well as those which are a current biological threat like influenza and Sars-CoV-2. Based at the University of Alabama at Birmingham, this center is a collaboration between multiple labs across the country, which allows them to combine their expertise in not only identifying small molecule compounds through methods like high throughput screening, but also testing the compounds effectiveness at inhibiting viral replication. Both of these steps are vital toward advancing a drug candidate into clinical trials. Many other members of the CETR, such as the Viral Immunotherapeutic Consortium at the La Jolla Institute for immunology, are similarly focused on developing vaccines for emerging zoonotic viruses such as Lassa and Ebola.
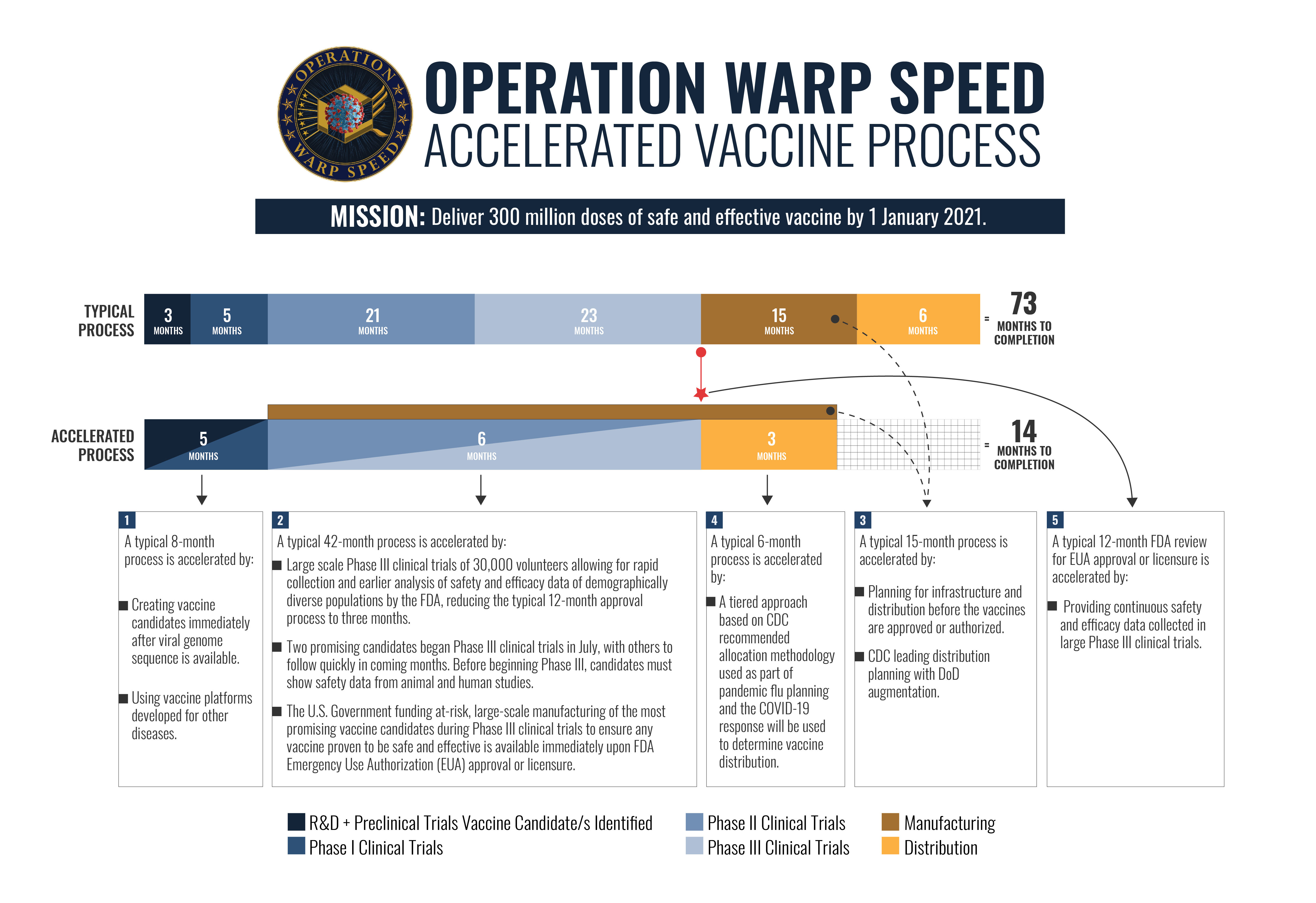
The speed and efficiency with which scientists and public health officials were able to develop and distribute vaccines in response to the Covid-19 crisis far exceeded prior expectations. The implementation of Operation Warp Speed (OWS), an initiative overseen by the Health and Human services department (HHS) as well as the Department of Defense (DOD), facilitated the speedy vaccine development by coordinating collaborations between public and private labs as well as by providing the capital needed to begin manufacturing of vaccines well before government approval. Likewise, global consortiums launching multi-billion-dollar initiatives and increased spending on projects such as the AD3C and CETR will undoubtably help to further decrease the length of time between the emergence of an epidemic and a meaningful therapeutic solution. However, the experience of the past year should be enough to convince anyone that even 1 to 2 years is too long to wait for a vaccine or drug during a pandemic. It is therefore essential that the US implement countermeasures in the form of policy and redistribution of funds that are commensurate with the magnitude of the threat.
The US federal budget for the fiscal year of 2020 allocated $41.68 billion to the entirety of the NIH, a budget that represents less than 7% of that given to the department of defense. The comparison may seem ridiculous to some, but I believe that emerging infectious diseases should now be conceptualized as an ongoing national security threat equal to that of terrorism or antagonism by foreign powers. Nearly 600,000 people have died of Covid19 in the US, which surpasses the number of US service member deaths in WWII, Korea and Vietnam combined. In my opinion, a massive increase in spending that can be used to fund a well-organized pipeline from basic research like the monitoring of potential zoonotic pathogens circulating in the wild to therapeutic development in both the public and private sector would serve as an investment that could ultimately save both lives and money. One way this could be accomplished is through the foundation of a federal office which directs funds through government grants to labs, both public and private, while conducting oversight to ensures that all labs within the system work synergistically to realize the overall goals of the program. As a country we cannot afford to wait for another deadly pandemic before we realize that, with sufficient funding and preparation, we can substantially reduce the amount of time it takes to respond to outbreaks and even prevent them from becoming epidemics in the first place.
Science Policy Around the Web March 25, 2021
By Andrew M. Wright, BSc

What’s in the huge pandemic relief bill for science?
The recently passed COVID-19 relief bill, or the American Rescue Plan Act of 2021, is a $1.9 trillion dollar economic stimulus package the primary purpose of which is to mitigate economic fallout from the coronavirus pandemic. To this end, there are funds designated for public health, namely $60 billion for vaccine manufacturing and logistics and $11 billion for international health aid. In addition, the package includes the following items for research:
- $1.7 billion to sequencing and track coronavirus variants such as the UK (B.1.1.7), South African (B.1.1351), and Brazilian (P.1) variants
- $600 for the National Science Foundation (NSF), which it can spend without constraints and will likely be used to some extent to disseminate grant funding
- $150 million for the National Institute of Standards and Technology (NIST), intended to be used for its advanced manufacturing division
- $100 million or the Department of Education’s Institute of Education Sciences for purposes of researching pandemic impacts on student learning and the effectiveness of various education strategies like remote and hybrid learning
- $95 million for the US Fish and Wildlife Service designated for prevention of zoonotic disease spread, ideally preventing future outbreaks (evidence suggests the novel coronavirus that causes COVID-19 could have been initially transmitted to humans from bats or pangolins).
While there have been significant losses in productivity and tax revenue for academic research institutions, no funding was provided to specifically bridge this gap. However $40 billion dollars was added to the Higher Education Emergency Relief Fund, and while half of that money is assigned to provide financial aid grants to student, the remaining money may help to offset pandemic related financial burdens at research Universities.
(David Malakoff, Science)
The impact of the COVID-19 pandemic on women’s health and gender equality
By Somayeh Hooshmand, PhD

The COVID-19 pandemic is a serious public health threat and has affected people globally. The coronavirus has unexpectedly disrupted our daily lives and threatened different aspects of life, health, and economy in the society. Life during this time has changed many routines and created new needs. Some changes are intermittent, while others create long-term effects. Therefore, it is essential to implement both immediate and long-term strategies to overcome the COVID-19 crisis and tackle its profound consequences.
While the coronavirus has had a profound effect on individuals, women, in particular, have come under increasing pressure due to several factors. The pandemic has affected the overall physical, social, emotional, financial and occupational health of women, which has intensified many existing social inequalities.
Gender inequality was a global problem long before the COVID-19 pandemic. In our society, women experience gender inequality in their lives through different times and cultures. A range of factors have been identified as drivers of gender inequality. For example, the Policy Brief: The Impact of COVID-19 on Women discusses the gap in earnings between women and men. Women’s saving is lower than men, and they hold less secure jobs than men over their lifetime. In addition, women make up most single-parent households, but they face disadvantages in social protection. One of the critical issues that the COVID-19 crisis has highlighted and brought to broader attention is gender inequality.
Numerous reports focus on the influences of pandemics on gender including the UN Secretary-General’s policy brief on the impact of COVID-19 on women and the UN Women’s “Spotlight on gender, COVID-19 and the SDGs.” In fact, the pandemic has exacerbated pre-existing gender inequalities in various domains, such as economic, social, political, and environmental life in many countries.
The pandemic reinforces existing social and economic disparity in society. The financial implications of the coronavirus pandemic illustrate that women were more likely to face negative effects than men. In more typical recessions, such as the one in 2008, men account for significantly more job losses than women. More men work in industries such as manufacturing and construction—the hardest-hit sectors during the recession. In contrast, more women lost their jobs compared to men during the COVID-19 outbreak. The pandemic has battered sectors with high female employment shares, such as the informal sector, domestic workers, home-based workers, street vendors, hospitality, tourism, restaurants, other food services, childcare, and health care.
According to the report “COVID-19 and gender equality: Countering the regressive effects,” almost two-fifths of all global labor is female, but the COVID-19 recession resulted in about half of the total job losses contributed to women. The report reveals that that women’s jobs are 1.8 times more vulnerable to this pandemic than men’s jobs. It appears that the COVID-19 pandemic has forced many women in these vulnerable groups to choose between their health and livelihoods.
Looking to the future, the impact of coronavirus on women’s finances and employment appears to reverse gains in gender equality and poverty alleviation in many countries. Policy responses must be immediate to alleviate the broad and damaging economic consequences of the pandemic for women. Several policy frameworks developed in United Nations, such as thematic policy briefs focused on COVID-19 focus on empowering women to achieve financial wellness.
Another factor that boosts gender inequality could be COVID-19’s disproportionate impact of unpaid caregiving, which is costly for women and for their families, health systems and economies.
The pandemic lockdown has put tantamount pressure on women by increasing family caregiving responsibilities due to school closures. They are still taking on most of the housework, raising and caring for children, and fulfilling familial duties without getting paid. New research shows that during COVID-19, the burden of specific, unexpected, and ongoing childcare responsibilities is disproportionately falling on the mother. In fact, the pandemic has shifted the balance in gender role expectations toward traditional norms and gender roles expected of women to care for other family members that had otherwise been redefined in modern society due to the social role of women.
In the face of this unprecedented pandemic, it is more critical than ever to have global, collaborative movement and policies about work/family balance to place women and girls at the center of COVID-19 recovery efforts as put forward by the United Nations in a call-to-action. There is an urgent need to increase awareness and discussion in society and inside homes, to distribute these responsibilities more evenly between men and women in order to take care of women’s physical, mental, and social health.
Gender inequality also manifests itself in the form of violence against women that raises serious concerns about women’s mental and physical health. Under normal circumstances, violence against women is associated with unemployment, cultural, mental, and economic factors, emotional dependence and insecurity, and social isolation and depression. These factors may contribute to poor mental health outcomes for women and may get far worse in the context of COVID-19 pandemic. Several studies show an increase in various forms of gender-based violence, especially domestic, psychological and sexual violence, in many countries since the outbreak of COVID-19. We must drive transformative change on women’s empowerment and gender equality to end violence against women by building a strong network of advocates and engagement of different factors during, and after the COVID-19 crisis.
In closing, I would like to argue that from the attitudes we have about gender identities and different set of ideas about gender roles to the policies we support in our communities, we can all take action to support gender equality throughout the COVID-19 outbreak. Now, as the world deals with COVID-19, we all are responsible not to let the pandemic set back gender equality. Attention to vulnerable groups including seniors, and women with disabilities, children and pregnant women, should be integrated with protecting women’s rights, strengthening social protection, education, health care, expanding women’s employment network, combating and eliminating violence against women.
46 days into the 46th U.S. presidential administration: 46 actions that support a return of science to the White House
By Katie Hudson, PhD
Biden has consistently promised to listen to scientists and “let the science speak”, a stark contrast from the previous administration. So far, he appears to be fulfilling that promise.

President Biden consistently promised before and after the 2020 election that he would lead with science by listening to scientists, let “science and truth” shape his policies, and pledged to restore “faith in America’s place in the frontier of science and discovery.” This was undoubtedly appealing to scientists leading up to the election, many of whom believed science was on the ballot. Science publishing organizations that typically stay apolitical suddenly felt the need to speak out prior to the 2020 election, often for the first time in their history, either to urge people against voting for Trump’s reelection (e.g. New England Journal of Medicine, Science, The Lancet), or going one step further to explicitly endorse Biden (e.g. The Scientific American – the first time it endorsed a candidate in its 175 year history, and Nature).
Many scientists were relieved at Biden’s election. The previous administration’s politicization of science has led to attacks on science, well-respected scientists, scientific integrity, and science-based policy. This has led to multiple science-related challenges that the Biden administration must address:
- Restoring Americans’ trust in science and the impartiality of federally-funded science agencies
- Combating misinformation that is contributing to public distrust in science, experts, and government
- A “staggering loss of government scientists” that has accelerated over the past 4 years: more than 1,000 scientists retired or quit, many of whom were not replaced, leading to a net loss of hundreds of federal scientists
In addition to these broad challenges, two more specific matters were on most scientists’ minds at the time of the 2020 election: the immediate concerns of the COVID-19 pandemic and the longer-term concerns of addressing climate change and the environment.
March 7th, 2021 marked the 46th day of the 46th U.S. presidential administration. Keeping with this theme, the following are 46 actions that have been taken by Biden and/or his administration since his inauguration that address the COVID-19 pandemic, climate change and the environment, or the other broad science-based challenges listed above that do not directly fit into the pandemic or environment categories:
COVID-19 pandemic
- Issued a 200 page ‘National Strategy for the COVID-19 Response and Pandemic Preparedness’ document to outline his specific plans to address the pandemic, stating “our national strategy will be driven by scientists and public health experts who will regularly speak directly to you, free from political interference as they make decisions strictly on science and public health alone”.
- Issued a first-day executive order to require mask-wearing on federal property and encourage “Masking Across America.”
- Issued a second-day executive order to mandate mask wearing on public transportation.
- Issued a first-day executive order to coordinate a government-wide COVID-19 response, including the creation of a paid Coordinator position in order to organize the response and also prepare for future biological and pandemic threats (the Trump administration has received widespread criticism for dissolving a directorate in 2018 that was created during the Obama administration to monitor and expedite federal responses to future potential infectious disease outbreaks like the COVID-19 pandemic).
- Promoted Dr. Anthony Fauci to the role of chief medical adviser, made him an active part of the COVID-19 response team, chose him to lead the U.S. delegation at WHO meetings, and removed restrictions on his ability to speak to the public. Dr. Fauci has served under multiple presidential administrations beginning with Ronald Reagan, is widely regarded as one of the nation’s top infectious disease experts, received the Presidential Medal of Freedom in 2008, and was (and continues to be) repeatedly undermined and attacked by Trump and his supporters. Fauci recently stated he often felt uncomfortable during the Trump administration and now feels liberated and free to speak without repercussions under the Biden administration.
- Invoked the Defense Production Act (DPA) to increase production of equipment and supplies for Pfizer’s COVID-19 vaccine, additional testing, and personal protective equipment for frontline workers.
- Invoked the DPA to accelerate production of the third COVID-19 vaccine under EUA. Merck will join their competitor Johnson & Johnson’s efforts to manufacture their COVID-19 vaccine, which led Biden to announce the U.S. will have enough vaccines for all U.S. adults by the end of May – two months earlier than the previous goal.
- Issued immediate inventory of COVID-19-related federal response supplies and identification of emergency needs to ensure a sustainable public health supply chain to local and federal governments.
- Established a data-driven response to COVID-19 and other future public health threats.
- Issued a multiple-part executive order to improve and expand access to COVID-19-related healthcare and treatments: establish the administration’s policy purpose, accelerate novel therapy development, improve the nation’s healthcare system capacity to address COVID-19, and improve access to healthcare.
- Extended federal support for state governors to use the National Guard in COVID-19-related responses and assistance.
- Created a task force to address inequalities and social inequities exacerbated during COVID-19. Many racial and ethnic minority groups are being disproportionately affected by COVID-19.
- Issued an executive order for the Department of Education to work with the Department of Health and Human Services to develop science-based guidelines to support the safe reopening of schools.
- Issued an executive order to protect workers from COVID-19 under the Occupational Safety and Health Act and direct the Department of Labor to issue new COVID-19 safety guidance for employers.
- Created a COVID-19 Pandemic Testing Board to coordinate and increase testing efforts across the country, including facilitating free testing for those without health insurance.
- Expanded Supplemental Nutritional Assistance Program benefits to address food insecurity during the pandemic.
- Expanded unemployment aid to cover workers who do not want to return to work due to their job or employer putting them at high risk of COVID-19.
- Ordered all government departments and agencies to identify actions they could further take to address crises caused by the pandemic.
- Invested $200 million for the CDC to expand genomics capabilities to aid in identifying the spread of emerging SARS-CoV-2 variants.
- Pledged to deliver 100 million COVID-19 vaccines to Americans in his first 100 days in office, which was initially thought to be an ambitious and potentially unattainable goal. As of his 46th day in office, 92,089,852 doses have been administered, indicating that this goal may be met early and potentially in half the time originally promised.
- Reinstated travel bans due to COVID-19, such as restrictions on travel from areas with emerging and more infectious SARS-CoV-2 variants.
- Purchased 8.5 million rapid at-home COVID-19 tests to increase national testing and used powers under the DPA to manufacture more tests.
- Visited the NIH to learn more about the developed COVID-19 vaccines and to personally thank the staff for their efforts.
- After the first month into the new administration, the CDC updated their mask recommendations and several other guidelines to be more consistent with expert recommendations.
- Launched a science-based advertising campaign to promote COVID-19 vaccines and awareness. A COVID-19 advertising campaign was planned during the previous administration, but it was cancelled in the fall of 2020 after an HHS review found it to contain propaganda aimed at promoting Trump’s reelection.
- Announced that free masks would be delivered to vulnerable areas of the country to provide masks for an estimated 12-15 million Americans.
- criticized states that recently decided to ease or completely remove COVID-19 precautions such as mask mandates, with Biden citing a failure of these states to follow the science. Epidemiologists and public health experts agree that the precautions were prematurely lifted.
- Biden’s $1.9 trillion COVID relief and economic stimulus bill that he proposed at the beginning of his term was officially signed into law March 11th. This bill is Biden’s first significant piece of legislation and is “one of the most consequential pieces of legislation in modern history,” according to House Rep. John Yarmuth. The bill is widely supported by the public: 70% of voters overall support the bill, with 41% of Republicans and 94% of Democrats in favor. Despite this, there was no Republican support in Congress and one House Democrat voted nay, leading to a narrow passage. The bill provides much-needed pandemic aid to Americans and local governments, is estimated to cut child poverty in the U.S. by half, and provides significantly more benefits to lower-income Americans and less to higher-income earners than the 2020 Trump pandemic stimulus bill, which conversely provided more benefits to higher-income Americans and less to lower-income earners. A bullet point summary of the major pieces in the finalized bill can be found here.
Climate change/environment
- Officially rejoined the Paris Agreement on February 19, 2021. An executive order and formal statement were released on the first day of his administration, though the terms meant it was not official for 30 days.
- Revoked the permit for the Keystone XL pipeline through a first-day executive order, citing an exhaustive 2015 review that concluded the pipeline would not benefit or serve the national interest with regards to energy security, economy, and the environment.
- Issued an immediate review of all agency actions taken during the previous administration to ensure they promoted the benefit of the environment, public health, national parks and monuments, workers, and communities.
- Halted oil and gas extraction leasing from the Arctic National Wildlife Refuge pending further environmental impact review.
- Directed federal agencies to account for the full costs of greenhouse gas emissions in cost-benefit analyses of regulatory proposals.
- Terminated the ‘emergency declaration’ for the southern border wall that was issued by Trump, thereby halting construction and funding of the US-Mexico border wall. The wall has negatively impacted the local environment and ecosystems, and was financed through improperly diverted funds from other agencies.
- Authorized plans to elevate climate change responses to be a national security priority, created the Office of Domestic Climate Policy, and created a national climate task force.
Other
- Rejoined the World Health Organization (WHO), reversing the one-year withdrawal process that began under the Trump administration in July 2020.
- Nominated a well-respected and decorated scientist, geneticist Dr. Eric Lander, to be his presidential science advisor and tasked Lander to “refresh and reinvigorate our national science and technology strategy.” Biden elevated this advisor position to Cabinet level for the first time in White House history, stating that “science will always be at the forefront of my administration”. This nomination has been well-received among scientists, though some have criticized this pick as a “[missed] opportunity to finally break the long lineage of white male science advisers”. Biden has pledged to ensure his administration is diverse and representative of the population, and has already nominated a record number of women and women of color.
- Issued an executive order to undo Trump-era executive actions that placed regulatory restrictions on federal agencies, which had led to inflexibility and reduced ability for federal agencies to respond to challenges (e.g. a requirement to discard two regulations for every one regulation proposed).
- Directed the Office of Management and Budget to modernize their regulatory review.
- Ordered all new appointees in every executive agency to sign an ethics pledge, commit to rejecting gifts from lobbyists, and to refrain from lobbying for at least 2 years after their term ends.
- Issued an executive order to strengthen federal employee protections by undoing Trump regulations that had lessened protections, such as a rule that made it easier to terminate civil servants. Whistleblowers, including pandemic response scientists, were often retaliated against during the Trump administration, despite the existence of legal protections.
- Issued a memorandum on restoring scientific integrity in government which calls for federal agencies to review current policies and adjust as needed to restore integrity and impartiality.
- Reestablished the President’s Council of Advisors on Science and Technology (PCAST) to advise him on science and technological information needed to guide public policy. Presidential science advisory boards began in 1933 with PCAST specifically established by President George W. Bush in 2001. Trump did not establish PCAST until almost three years into his administration, with the group’s purpose narrowed to primarily focus on the private sector and the economy.
- Revoked restrictions on federal workplace diversity training that were implemented during the Trump administration.
- Appointed a CDC director that has promised to communicate science and truth with the public, as well as to remove the “muzzle” from CDC scientists.
- Retained Dr. Francis Collins as the NIH director, who was first appointed when Biden was Vice President in 2009. Collins is a well-respected physician and geneticist who previously directed the National Human Genome Research Institute at NIH from 1993-2008, was instrumental in leading the Human Genome Project to completion, and is the only presidentially appointed NIH director to serve more than one administration.
While the new administration has been busy, much work still remains. No significant action has been taken, or even proposed, to combat the overall problem of misinformation. A recent survey found that less Americans are hesitant about receiving a COVID-19 vaccine than they were a few months ago, but 30% still indicate they would refuse a vaccine – potentially keeping us below the rate needed for herd immunity. Biden outlined plans in his pandemic response blueprint for science-led public education campaigns to combat COVID-19 misinformation such as that revolving around vaccines, which is a step in the right direction. However, this may fall on deaf ears as there has been growing public distrust of the government and the media in recent decades. Willingness to take or implement recommended COVID-19 precautions like wearing a mask have unfortunately been plagued by political partisanship, with Trump’s supporters often refusing to follow COVID-19 recommendations. After he lost the 2020 election, Trump repeatedly made false claims of a rigged election and there was a significant spread of misinformation that supported these false claims (e.g. videos on YouTube and other social media sites). Poll after poll has shown that the majority of voters from the Republican party believe the 2020 election was fraudulent, despite no credible evidence, with a significant portion of voters who still believe Trump won the election. Why should we expect these individuals to believe any information coming from an administration whom they believe cheated and was not rightfully elected?
Combating misinformation is a complex issue that cannot be addressed in the remainder of this article. It would require careful legislation and considerations, as many solutions (e.g. stricter regulations for social media and the internet) might be seen as infringements on the First Amendment’s right to free speech. Our education system should be doing a better job of teaching our youth how to think critically and discern fact from fiction – perhaps taking lessons from Finland, which starts teaching children early and is considered one of Europe’s most resistant nations to false information. Regardless, the current administration needs to do much more than it is currently doing.
A few small steps have been taken to return integrity and impartiality to government science, but continued action is needed, and time – much longer than 46 days – will tell if scientists make a return to federal government positions. Qualified, diverse, and early-career scientists need to be heavily recruited to federal positions. Agency leadership and policies need to foster retention of current staff members. Scientists need to be reassured that they will not have their work or communication with the public restricted or contradicted by politics. A detailed roadmap with recommendations written by the Union of Concerned Scientists can be found here.
We have rejoined the Paris Climate Agreement, but more aggressive action is needed. Biden outlined calls for more aggressive action in his climate plan and his intentions to push other international leaders to do the same. States across the country also need to commit to action, with some local leaders still needing to accomplish the first step of admitting that climate change is real and is caused by human actions.
Science is off to a good start in the Biden administration, but we still have a long way to go. And as this article ominously states: it could take decades to recover.
Containing Zoonosis: global threats require global unity
By Atul Gopal, PhD

Humanity is currently facing multiple global crises: climate, energy, and pathogenic diseases. With the rise of COVID-19, a renewed emphasis has emerged on prioritizing a global approach for preventing, containing, and treating zoonotic disease. Despite this, individual countries remain hesitant to share their resources and shoulder the economic burden to institute a global strategy to prevent future pandemics.
Zoonoses (diseases or infections naturally transmitted between people and vertebrate animals) accounts for one billion cases of illness and millions of deaths every year. Over 30 new pathogens have been reported globally in the last three decades, resulting in zoonotic diseases like Rift Valley Fever, Yellow fever, and, most recently, Zika and COVID-19. Infectious diseases can spread faster than ever before due to increases in globalization (i.e. international travel and trade). Additionally, exponential increases in the human population continues to profoundly alter the planet’s geosphere and infringe on the habitats of most other species. As a result, the probability of newer zoonotic diseases spilling into the human population has also increased, resulting in an inevitable subsequent pandemic. Hence, clear interventions on a global scale are required to effectively combat this crisis.
The recent COVID-19 pandemic has demonstrated that we do not live in isolation; our behavior as individuals or as nations play a significant role in fueling or fighting the pandemic. The global connectedness of our modern age makes us more vulnerable. The Center for Disease Control and Prevention states that “a pathogen can travel from a remote village to major cities on all continents in 36 hours.” The magnitude of solving the problem of future pandemics is so huge that no country can tackle this alone. Instead, a concerted global effort is required. It is time to transform the global connectedness that we share now to our advantage through mutually beneficial international collaborations.
Science Diplomacy may play a significant role in this process. International relationships can be fragile, traditionally being rooted in the realm of national security, and, therefore, more susceptible to political upheavals. Science offers a new avenue of collaboration that is both apolitical and universal in nature, offering a path to strengthen previously strained relationships. For example, the collaboration between the USA and the Soviet Union during the heights of the Cold War, the Apollo Soyuz Test project, led to the development of a ‘docking’ system crucial for accessing the international space station, and it is still in use today. Science diplomacy opens avenues to tackle global problems, including zoonoses, which are out of reach for a single nation to address. A global pandemic surveillance and preparedness network is an excellent avenue for science diplomacy to thwart the treat of future pandemics.
Organizations like the World Health Organizations (WHO) play significant roles in fostering international collaborations for pandemic preparedness. WHO has adopted a comprehensive ‘ONE HEALTH” approach that recognize that “the health of people is closely connected to the health of animals and our shared environment.” WHO has prepared a “Global Influenza Strategy 2019-2030” to prevent, control and prepare for an influenza pandemic, which many consider as the greatest threat to global public health. The main mission of this plan is to ensure that “WHO countries and partners collaborate to optimize and align global and national capacities for prevention, rapid detection and response, to reduce the burden and impact of seasonal, zoonotic and pandemic influenza.” Strengthening the global surveillance as well as timely and transparent sharing of data is an integral component of this plan and can be only facilitated with cooperation and collaboration between all the WHO member nations.
One major obstacle in implementing an effective global surveillance system is the inequality between member nations. The variations in health system’s capacity within different member nations is a significant risk factor for detecting the emergence and containing the spread of zoonotic infectious diseases. Many developing countries lack the infrastructure and resources needed to effectively handle an outbreak because they are already burdened by their fragmented health systems, lack of laboratory and diagnostic capacity, trained scientific labor, etc. Hence, it is of great importance that, with the cooperation of developed economies, developing countries enhance their scientific infrastructure to effectively prevent future pandemics.
Currently, the economic burden of combatting pandemics must be shouldered by the more developed economies of the world. A recent study estimated that approximately 344 billion dollars is needed to optimally implement a proactive global strategy for mitigating future pandemics. This strategy, if implemented within the next 27 years, can reduce the rate of pandemics by 50% and save more than 360 billion dollars compared to the current reactive strategy (i.e. responding after an outbreak). This study further highlighted that the timelines for implementing these measures are more urgent than climate change. Given that each country is responding to the COVID-19 pandemic on their own soil and trying to rebuild their individual economies, investing in global pandemic projects may not be a high priority. Despite this, it is of grave importance that developed economies take action in this global endeavor. It is time that zoonotic diseases are recognized as a major security threat to the well-being of the nation. If nations consider pandemic preparedness as a matter of national security, then millions of dollars could be set aside for that purpose and allocated to tackle future pandemics. Contrary to the conventional national security measures that strengthen armed forces, tackling the threat of zoonotic diseases require the strengthening of scientific infrastructures. Instead of guns and missiles, investments should be made to procure pipettes and microscopes. Instead of being trained for war, men and women should be trained to run biological assays and perform genetic sequencing. If we collaborate with other nations to prepare and ‘arm’ ourselves with transparent and effective global scientific infrastructure, borders can be secured, lives can be saved, and economies can flourish — worldwide.

{kind=link}